
Currently The Scored Patient-Generated Subjective Global Assessment (PG-SGA©) sets the standard of and is the preeminent interdisciplinary patient assessment (weight, intake, symptoms, functional status, disease state, metabolic stress and nutritional physical examination) in oncology and other chronic catabolic conditions.
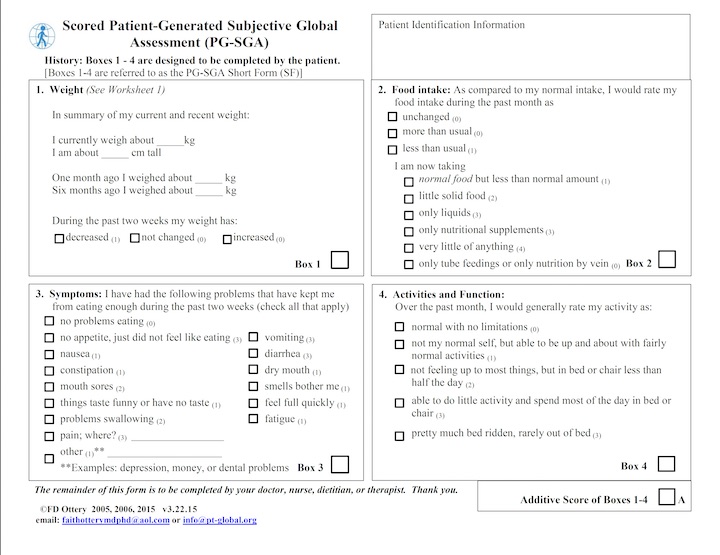
The Scored PG-SGA© includes the four patient-generated historical components (Weight History, Food Intake, Symptoms and Activities and Function – also known as the PG-SGA Short Form©), the professional part (Diagnosis, Age, Metabolic stress, and Physical Exam), the Global Assessment (A = well nourished, B = moderately malnourished or suspected malnutrition, C = severely malnourished), the total numerical score, and nutritional triage recommendations. Subsequently, the Scored PG-SGA© allows for triaging of specific nutrition interventions, as well as facilitating quantitative outcomes data collection.
Patient-generated
The first four boxes of the PG-SGA© (Weight history, Food Intake, Symptoms and Activities and function; which are the screens Patient, Weight, Food Intake, Symptoms and Activities in the Pt-Global web tool©) have been designed to be used by the patient independently. This patient-generated aspect has been chosen for two reasons: 1) Appropriate Use of Professional’s Limited Time and 2) Patient Involvement – identification and empowerment, because involvement of the patient gets to the core of the problem. Obviously there may be some situations where this may be impossible currently, e.g., severe visual deficit, inability to read, or lack of availability of the relevant patient language. However, short of these impediments, it is always preferable for the patient to complete the PG-SGA©, particularly in the context of their eating/intake, their symptoms (that they may not tell the family, nurse or physician but that do impact ability to eat and absorb adequate macro- and micronutrients), and functional status.
In Box 1 (Weight history) and Box 3 (Symptoms) scores are additive, whereas scores of Box 2 (Food intake) and Box 4 (Activities and Function) are not. In these boxes the highest point score should be used.
Professional component
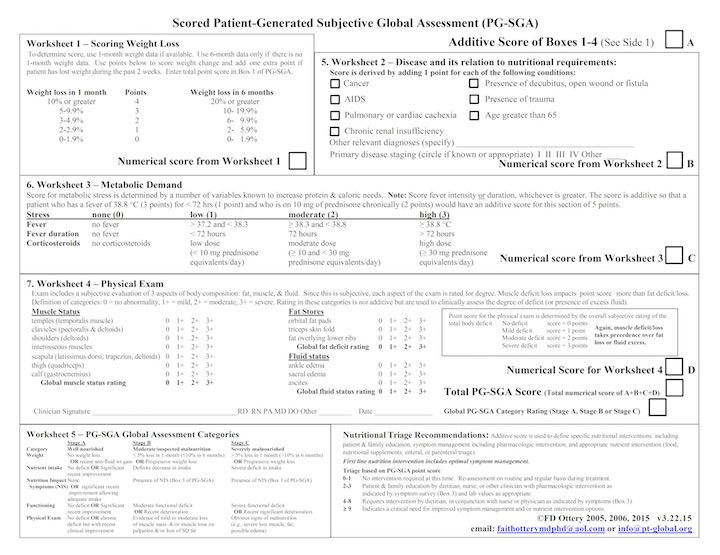
The remaining portions of the PG-SGA© (Professional screens in the Pt-Global web tool©) are to be completed by the professional (physician, nurse, or dietitian). The professional part, in a pilot study at Fox Chase Cancer Center, added less than l minute to the overall patient assessment process. The disease and its stages are known to the evaluating clinician. Components of metabolic stress can include sepsis, neutropenic fevers, tumor fever, biologic response modifier of therapy (e.g., interferon), or use of corticosteroids.
Physical components include loss of subcutaneous fat (e.g., triceps region and midaxillary line at the level of the lower ribs), muscle wasting (e.g., temporal areas, deltoids, and quadriceps with a loss of bulk and tone by palpation), and edema (e.g., ankle or sacral) or ascites.
Anabolic vs. catabolic
Throughout the use of the PG-SGA© or the Pt-Global web tool©, it is important to think of the patient in terms of whether the patient is anabolic or catabolic. Lean tissue/non-fluid weight increase tends to represent anabolism (positive nitrogen balance) whereas lean tissue/non-fluid weight decrease may represent catabolism in an ill patient.
Weight information is addressed along a continuum – 6 months (chronic), 1 month (intermediate), and past two weeks (acute) change. For example, if the patient’s weight is 100 lbs or 100 kg at 6 months and then decreased by 10% or increased by 10% (e.g., from 100 lbs/kg to 90 lbs/kg or 110 lbs/kg, respectively), the weight that is more recent lets you know what is going on more recently in terms of the patient metabolically in an intermediate setting. If weight decreased, perhaps this is related to treatment or poor symptom control. If increased, perhaps it is related to excellent intervention by the professional, to stop what had previously been uncontrolled disease or treatment related weight loss.
The previous two weeks is a gauge of what is going on in the patient now metabolically or physiologically. One uses the 1 month weight, if available, since it represents the intermediately chronic situation for which there are data regarding the prognostic implications.
Physical exam
Performance of the physical exam is not mandatory but is important. The scoring of the PG-SGA© and the algorithm that supports the Pt-Global web tool© is based on the preponderance (generally 80-90%) of the total PG-SGA score being based on the patient-generated aspects (e.g., Boxes 1-4 of the original PG-SGA© and the patient component of the Pt-Global web tool© (Patient, Weight, Food Intake, Symptoms, and Activity). The patient-generated aspects are also referred to as the PG-SGA Short Form© (SF) or the abridged PG-SGA©.
It is important to note that the total score of the physical examination is 3 points – so that even if one was not certain that the deficit was moderate vs severe or mild vs moderate, the difference would only be 1 point. Many find the appreciation of this as lessening some of the intimidation of doing the physical exam. The other aspects of the professional components of the PG-SGA©/Pt-Global web tool© are the presence of fever, fever duration and use of corticosteroids. Each of these variables can have significant acute or chronic effect on muscle mass and patient function.
These variables must be taken into consideration in the assessment of your patient, even if you only utilize the PG-SGA Short Form© (Boxes 1-4). For example, if the patient has a score of 7 points but is on corticosteroids or has a fever, this should make the professional address the intervention based on a higher score than that captured with the data based on Boxes 1-4 of the PG-SGA©.
Additional insights by physical exam
Also, appreciation of components of the physical examination can give additional insight. For example, the distribution of the loss of muscle mass can be important. If the patient is spending most of her/his time in bed or chair, the muscle loss you see below the waist will be a combination of disuse atrophy plus malnutrition, whereas that above the waist tends to be more prominently related to malnutrition.
Also, while not specifically part of the PG-SGA©, when one is examining the patient, there may be markers of specific nutritional deficiencies that can also be appreciated, e.g., scaly dermatitis of zinc deficiency (and poor wound healing) in the patient with chronic high volume GI losses or a similar scaly dermatitis of essential fatty acid deficiency in a patient who a clinician chronically failed to order lipids with the patient’s parenteral nutrition.
Numerical PG-SGA score
The PG-SGA© was originally developed as a continuous rather than categorical assessment, whereas originally the SGA was considered a categorical assessment (A = well nourished, B = moderately malnourished or suspected malnutrition and C = severely malnourished). The PG-SGA score is based on all data completed, from weight history up to and including the physical exam (all screens from Patient up to and including the Professional screens in the Pt-Global web tool©).
The numerical PG-SGA score provides professionals with clearer guidelines as to the level of medical nutrition therapy needed in a given case, while the A, B, or C rating provides an overall picture of a patient’s current status.
How the numerical PG-SGA score relates to the PG-SGA Category score
Although the numerical PG-SGA score and PG-SGA Category score are related, they are independent assessment and triage systems. In general, the higher total additive scores upon initial exam correlates with more severely malnourished cases. An example of a high numerical score that does not correlate with a severely or even moderately malnourished rating is the patient who is seen for the first time, and receives a numeric score of 15 and has a subjective global rating of C (severely malnourished). The same patient subsequently receives the appropriate medical nutrition therapy and pharmacologic intervention for nutrition impact symptoms. Upon subsequent follow-ups, the patient is considered to be anabolic (increase in non-fluid weight with improved intake, improved symptom management, etc.), which is PG-SGA Category A, though the physical exam suggests moderate to severe depletion.
Multiple languages
The original English PG-SGA© has been translated and culturally adapted for the Dutch, (European) Portuguese and Thai setting and various other langauges. Currently available language versions of the PG-SGA are available as download on the Pt-Global website.